Introduction
As defined by American Heart Association, Cardiac Death is occurring within one hour from the onset of symptoms. It affects 20% of Western Countries population.
Under current clinical practice, we evaluate and treat with only a small high-risk population of cardiac arrest survivors and a tiny fraction of other risk groups.
If we are to make a substantial impact on total death mortality, we must begin to evaluate and treat larger groups at risk.
To simply double the number of sudden death we could potentially prevent, we must go to evaluate and treat million of patients with congestive heart failure.
Given current constraints on costs, clearly not all these patients will get invasive Electrophysiology Study (EP) and not all get ICDs. Some high predictive non invasive tests are therefore required to determine who will benefit most from invasive study and definitive treatment.
Many different
types of Risk Assessment Methods have been proposed up to now but they either
lack adequate sensitivity to identify most of those at risk or lack aguate
positive predictive value to justify definitive treatments (Table 1) 1-4
|
Predictor |
Source |
Sensitivity |
PPV |
|
LVEF<0.4 |
Pedretti, 1993 |
79% |
26% |
|
LVEF<0.4 |
Bourke, 1991 |
73% |
6% |
|
SAECG |
Pedretti, 1993 |
79% |
17% |
|
SAECG |
Farrel, 1991 |
64% |
17% |
|
HRV |
Pedretti, 1993 |
89% |
15% |
|
HRV |
Farrel, 1991 |
92% |
17% |
|
HRV-2 Powers vars |
Bigger, 1996 |
20% |
80% |
|
NSVT |
Pedretti, 1993 |
42% |
25% |
|
NSVT |
Farrel, 1991 |
56% |
15% |
Table 1:Different types of Risk Assessment Methods
____________
For correspondence:
Daniele Marangoni Dr. Eng. Vicolo S. Franc. al Corso 4, 37122 Verona, Italy
E-mail:
marangon@easynet.it
T Wave Alternans Background
Electrical Alternans represents a variation in the morphology of electrocardiographic complexes on every other beat.
Visible Alternans of the electrocardiogram is often associated with pericardial effusion. True electrical Alternans results from an alternation in electrical conduction patterns and is believed to be associated with Alternans of repolarization at cellular level.
It appears as an alternation in the morphology of the T wave and it is called T Wave Alternans (TWA).
Electrical Alternans was reported in the literature since 1909 and there have been many cases reported (Figure 1) 5
Figure 1: Relaxed (left) and Emotional Exitement (right) Visual TWA in LQTS Patient
Despite the clinical association reported in literature, the consensus view until recent years has been that Alternans is an electrocardiographic curiosity rarely encountered in clinical practice.
Interestingly Kalter 6 found that TWA was associated with very high mortality rate of 61%.
In 1984 Joseph Smith and Richard Cohen working at MIT, published results of their computer simulation of ventricular conduction process using a model incorporating dispersion of refractory times. In the course of their studies, they observed electrical Alternans preceded the onset of VT 7
On the basis of computer simulation, the investigators realized that electrical Alternans might be a useful clinical marker of susceptibility to ventricular arrhythmias. However, since it was rarely seen on the electrocardiogram, they hypothesized that it was often present but simply too small to be seen.
Spectral Method
The Spectral Method was developed to detect leads of Alternans too small to be seen on ECG.
In this method, the amplitude of corresponding points on the T wave is measured in 128 consecutive beats. The resulting time series is analyzed using a Fast Fourier Transform method to obtain the power spectrum of the fluctuations.
Because the measurements are made once per beat (instead of once per second), the x-axis of the power spectrum is measured in frequency units of cycles per beat instead of more usual cycles per second.
Alternans shows up as a peak at exactly 1 cycle every 2 beats therefore at 0,5 Cycles / Beat.
Using this Spectral Method, Alternans may reliable be measured at level of one microvolt in presence of low noise ECG recordings.
The actual method is more complicated. To obtain a measurement of T Wave Alternans over the entire T wave, multiple Power Spectra corresponding to sequential points on the T wave are computed.
To test the Spectral Method, Joseph Smith and Richard Cohen 8 measured electrical Alternans in dogs during a variety of interventions, and compared these measurements with changes in ventricular fibrillation threshold.
In nornothermic animals, the level of Alternans remains at the same low level over a wide range of heart rates. However, in the hypothermic animals, the level of Alternans rises progressively with increasing heart rate, until spontaneous ventricular fibrillation occurs.
In a set of about 120 paired measurements of Alternans and ventricular fibrillation threshold, there was a clear relationship between TWA and lowered ventricular fibrillation threshold .
Heart rate Dependence of TWA
There is a typical relationship between Alternans and heart rate in arrhythmia risk patients undergoing exercise stress. Alternans appears when the heart rate exceeds a patient specific threshold, usually between 90 and 110 beats per minute; the Alternans increases with increasing heart rate above that threshold. During recovery, Alternans disappears as the heart rate drops below the threshold.
One way to increase the heart rate noninvasively is exercise testing.
However, under normal conditions, the high levels of artifacts obtained during exercise, make the measurement of microvolt level Alternans, very difficult. This problem is solved by the use of High-Resolution (Hi-Res, Cambridge Heart Inc. Boston) electrodes.
Hi-Res
Electrodes use multiple segments and proprietary signal processing to
substantially reduce motion artifact through a process called adaptive
cancellation.
Fig 2 High Resolution Electrodes
These advances make TWA be able to be analyzed at the end of an Ergometer Stress Testing with the CH2000 (Cambridge Heart Inc. Boston).
Testing Procedure
The procedure is similar to a standard stress test.
The electrodes hook up of the patient requires:
7 standard and 7 Hi-Res Electrodes (Standard +XYZ). The CH2000 is able to measure and display:
· the electrodes impedance per each electrodes (skin abrasion is required to have low impedance)
· the muscular noise per each electrode ( it is important to avoid positioning of electrodes on muscular parts)
· ECG detected on each electrodes compared to reference (for a visual check of the ECG quality per each electrode as well as per each lead).
The test requires low increase of Watt loads per each stage to avoid sharp increase of Heart Rate. The CH2000 controls the Revolution Per Minute (RPM) of the Ergometer pedaling and compares to the Heart Rate to avoid pedaling rate of ½ of HR that could produce false Alternans; it controls exercise Noise Level in real time, Bad Beats (arrhythmias and artifacts). When the Heart Rate reaches 105 for 2 minutes (a bar indicates the signal acquisition) the TWA test is considered conclusive and the nurse/physician can decide to stop the test or to continue for a submaximal/maximal standard 12 leads ST test.
The CH2000 provides high-resolution 12 leads display, laser printout and capability to review and edit full disclosure ECG and at the same time see the actual patient ECG for unstable patient continuous monitoring.
At the end of test a complete ST standard report and a TWA report are printed.
The TWA report includes:
· HR trend with instant HR changes and mean trend
· Bad beats, Noise trend
· Alternans (peak at 0,5 with noise ratio) trend in VM, X,Y,Z and precordial leads
· RPM, Respiration, Delta HR, RR trend
TWA test is considered positive if Sustained TWA is >1.9mV (with a Signal/Noise ratio >3) for more than one minute and the with TWA onset < 110 Bpm. Alternans has to continuous increase with HR and has to decrease with HR to be considered Sustained.
Automatic interpretation will be implemented soon.
Published Clinical Studies
In a landmark paper published in the New England Journal of Medicine in 1994 9, David Rosenbaum, Jeremy Rusckin and Richard Cohen conducted a prospective clinical study of the efficacy of TWA in predicting arrhythmic events in 83 patients undergoing Electrophysiology testing.
All comers to Electrophysiology laboratory were studied. The level of TWA was measured during atrial pacing at 100 beats per minute and it was compared with 2 clinical endpoints: the inducibility to sustained ventricular tachycardia or fibrillation during programmed stimulation (EP study) and secondly, arrhythmia-free survival.
There were 15 patients being evaluated for supraventricular arrhythmias and a total of 20 patients had no known organic heart disease. These patients served as internal control for the study.
TWA predicts EP results with a sensitivity of 81% and specificity of 84%. In predicting arrhythmias -free survival sensitivity was of 89% and specificity of 89%. These results were each high significant (p<0.001).
Patient who were TWA negative had 95% arrhythmia-free survival rate at 20 months, whereas those patients who were TWA positive had only 20% arrhythmia-free survival rate. The results were almost identical for EP study.
One of the limitations of the Rosenbaum study was that the HR was increase using Atrial pacing. In order to make it completely non-invasive diagnostic test exercise was used. Two papers in 1997 demonstrated that exercise produced equivalent results to Atrial pacing. 11
In a study of 27 patients Mark Estes, Douglas Zipes and Nabil El-Sherif demonstrated that exercise TWA predicts EP with accuracy similar to Rosenbaum results. 12
The fist major study to confirm the NEJM study was conducted by Stephen Hohnloser 13
95 consecutive patients receiving ICD were included in the study.
They underwent a battery of risk stratification tests including TWA, EP study, LVEF, Baroreflex Sensitivity, Signal Averaged ECG, Heart Rate Variability, QT dispersion, RR variability and Non-Sustained Ventricular Tachycardia.
The endpoint of the study was appropriate discharge of the ICD. Characteristic of this high-risk patient population includes a median ejection fraction of 36.
More than 2/3 had coronary artery disease.
Figure 3
TWA was the best non-invasive risk predictor in this population. Ejection fraction was the only statistically significant predictor.
The Kaplan Mayer survival curve shows those patients tested TWA negative had 80% event free survival after 18 months (Figure 3). Those that tested positive had less than a 40% event free survival over the same period of time.
TWA was more predictive of appropriate ICD firing than EPS in this population. Although there was a trend toward significance with EPS, EPS did not reached statistical significance probably due to the fact that about 40% of the patients were VF patients.
In the coronary disease sub-group the separation of the curves for TWA is even more dramatic with a 23% survival rate at 18 months.
New Clinical Studies
Michele Gold acted as the principle investigator of the TWA multicenter trial including Nabil El-Sherif group, which was designed to expand TWA claims. The study compared TWA, SAECG and EP as predictors of events during follow-up. 14
There were 2 end points: the primary endpoint was "ventricular tachyarrhythmic events" defined as resuscitated VT, VF and sudden death. The second was "resuscitated VT, VF and total mortality.
These studies were presented at the AHA in Nov. '98 and updated at ACC in March '99. The 272 patients in the study were weighted toward elective EP study, generally for syncope and presyncope. Only 27% of the patients had documented arrhythmia; 43% has suspected VT and 15% had suspected SVT.
As all previous studies, TWA was predictive of ventricular arrhythmic events and documented sudden cardiac death. In particular as predictor of VT/VF and Total Mortality the relative risk for TWA was 11 (p<0.001) compared to 2 of SAECG (n.s.) and 3 (p<0.01) of EPS.
In another study developed in Frankfurt presented at AHA 15 in Nov.98, 107 patients with class II and III congestive heart failure (CHF) with no prior history of VT/VF had a follow up of 2 years with endpoint resuscitated VT/VF and Sudden Death (Figure 4).
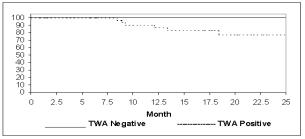
Figure 4
Risk stratification performed: TWA, LVEF, BRS, SAECG, HRV, QT Dispersion mean RR, NSVT. EPS was not performed in this group. 58% had coronary artery disease.
The preliminary results in 81 patients show TWA to be the only significant predictor. No patient who tested negative for TWA had an event within 24 months of follow up, providing a sensitivity of 100%. The positive predictive value was 23%.
These results in CHF patients were confirmed in a paper presented at
the Italian Congress of Cardiology by Pedretti showing a sensitivity of 100%
and a positive predictive value of 42%. 16
Conclusions
In summary, tree studies demonstrate TWA to be as good a predictor of Ventricular Events as EPS in a EP population. The Frankfurt study showed TWA to be highly significant predictor in the heart failure population. The manuscript has been submitted for publication.
The possibility to have a non-invasive Risk Stratification Method with very high Sensitivity and reasonable good Positive Predictive Value to be used in a specific and growing population as Congestive Heart Failure patients, makes TWA a very important screening clinical tool to select patients for additional invasive diagnostic testing and antiarrhythmic therapy
as ICD implantation.
Due to actual constraint on costs, the possibility to avoid expensive invasive diagnostic tests in patients with CHF and TWA negative test, makes the TWA test during a standard 12 leads ECG Stress Test for ST evaluation, cost effective. In the future TWA could eventually become a clinical tool for a broad and lower risk population group as soon as other ongoing studies in other lower risk population will provide the same evidence as with CHF patients.
References
3. Pedretti R. Etro MD, Laprota A, Braga SS, Caru B, Prediction of late arrhythmic events after acute myocardial infarction from combined use of non-onvasive prognostic variables and inducibility of sustained monomorphyc ventricular tachycardia. Am J Cardiol 1993;71:1131-1141
4. Bigger JT Jr, Steinman RC, Rolnizky LM,Fleiss JL, Albrecht P, Cohen RJ, Power law behavior of RR-interval variability in healthy middle-aged persons, patients with recent acute myocardial infarction, and patients withheart transplants. Circulation 1996;93:2142-2151
5. J.P.Schwartz, Malliani Am Journal of Cardiology 1975
6. Kalter HH. Electrical Alternans, NY State J. M. 1948
7. Smith and Cohen PNAS; 81: 233-237
8. Smith JM, Clancy EA, Valeri CR, Ruskin JN, Cohen RJ: Electrical Alternans and Cardiac Electrical Instability. Circulation 1988;77:110-121
9. Rosenbaum DC, Jackson LE, Smith JM, Garan H, Ruskin JN, Cohen RJ. Electrical alternans and vulnerability to ventricular arrhythmias. N Engl J Med 1994;330: 235-241
10. Pastore JM, Girourard SB, Rosenbaum DS, Mechanism of initiation of ventricular fibrillation during T-wave alternans. PACE 1997;20:1196A
11. Hohnloser SH Klingenheben T, Zabal M, LiYG, AlbrectP, Cohen RJ. T-wave alternans during execrcise and atrial pacing in humans. J Cardiovacc Electrophysiol 1997;8: 987-993
12.
Estes MNA,
Michaud G, Zipes DP, Nabil El-Sherif et al. Electrical
Alternans during rest and exercise as predictor of vulnerability to ventricular
arrhythmias. Am J Cardiolog 1997; 80: 1314-1318
13. Hohnloser SH, Klingenheben T, Li YG, Zabel M, Cohen RJ. T Wave Alternans as a Predictor of Recurrent Ventricular Ventricular Tachyarrhythmias in ICD Recipients. J Cardiovasc Electrophysiology 1998; 9: 1258-1268
14. Gold MG, Bloomfield DM, Anderson KP, Wilbert DJ, El-Sherif N, Estes
NAM Groh WJ, Kaufman E, Cohen RJ. A comparison of T Wave Alternans, Signal
Averaged ECG, and Electrophysiology Study to Predict Arrhythmia Vulnerability JACC February 99
15. Klingenheben, Cohen RJ, Hohnloser S. Predictive Value of T Wave Alternans in patients with Congestive Heart Failure Supplement to Circulation Vol 98 ;17:I-864
16.
S. Sarzi Braga, R.
Tramarin, R.F.E. Pedretti. Significato Prognostico della TWA in Pazienti CHF, Giornale Italiano di Cardiologia May
1999